





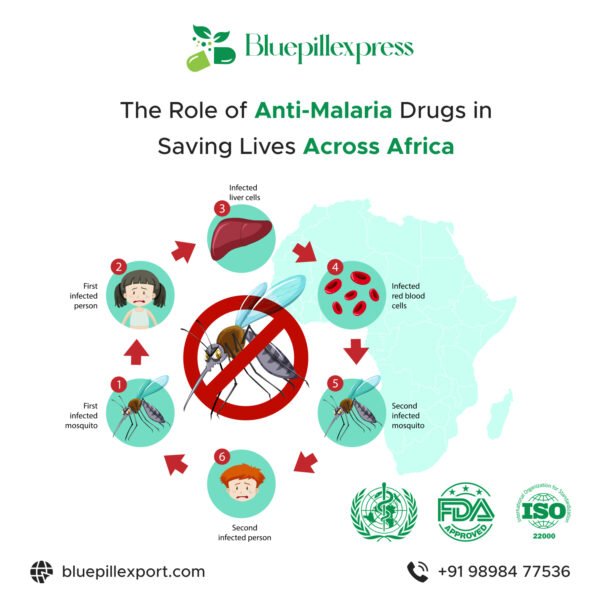
How Africa Is Winning the Battle Against Malaria with Modern Medicines
Malaria has been an ancient, persistent burden across sub-Saharan Africa. Yet over the past two decades the continent has seen some of the most important breakthroughs in prevention and treatment the disease has ever seen. While progress has not been linear—recent years have shown stagnation and even upticks in cases—there’s a clear and growing set of tools and strategies built on modern medicines that are changing outcomes for millions of people. This article explains how those medicines and campaigns are working in practice, the science behind them, and what must happen next to keep momentum going. World Health Organization+1
A new era of malaria vaccines: protecting children at scale
The single biggest paradigm shift of the last five years is the arrival of malaria vaccines that can be delivered at scale to young children—the group most at risk of dying from the disease. RTS,S (first recommended by WHO in 2021) and the R21 candidate both proved in trials that vaccination can cut clinical malaria and severe disease in children and are now being introduced in national programs across multiple African countries. Early rollout data and modelling show that vaccine deployment, when combined with existing tools, reduces hospitalisations and deaths among infants and toddlers. World Health Organization+1
Why this matters: vaccines add a layer of protection that reaches children who might not sleep under nets or access care in time. They are not a replacement for bed nets, chemoprevention, testing or treatment—but they tilt the risk curve for the youngest and most vulnerable. Implementation lessons (delivery through routine immunization schedules, community engagement and cold-chain logistics) have been learned rapidly from pilot countries and are now being scaled. World Health Organization
Seasonal malaria chemoprevention (SMC): a low-cost, high-impact preventive medicine
Seasonal malaria chemoprevention (SMC) is a targeted preventive strategy that gives full therapeutic courses of antimalarial drugs to children (typically 3–59 months) during the months of highest transmission. In the Sahel and other highly seasonal zones, SMC has become a public–health staple because of its simplicity and proven impact. Large operational studies and WHO guidance show that SMC, when correctly administered across multiple cycles each transmission season, substantially reduces clinical cases and hospital admissions in young children. Malaria Consortium+1
Recent programmatic innovation has expanded SMC’s reach and evaluated different drug regimens (for example sulfadoxine-pyrimethamine plus amodiaquine — SP+AQ — and trials of dihydroartemisinin–piperaquine as an alternative). Those innovations are helping countries tailor chemoprevention to local resistance patterns and season length, boosting effectiveness. The Lancet+1
New and next-generation antimalarial drugs: staying ahead of resistance
Drug resistance has always been the Achilles’ heel of malaria control. Artemisinin-based combination therapies (ACTs) are the standard frontline treatments today, but parasites can evolve resistance to partners and—worryingly—there are signs of reduced efficacy in some regions. The scientific and pharmaceutical communities have responded by accelerating development of drugs with new mechanisms of action.
Notable advances include candidate compounds such as ganaplacide (KAF156) and cipargamin (KAE609), both of which work differently from artemisinins and have progressed through late-stage clinical testing. Ganaplacide combined with lumefantrine showed positive trial data in children and adults, and is being evaluated in Phase III studies — a potential alternative if ACT efficacy declines. Cipargamin’s intravenous formulations are being developed for severe malaria. Broad discovery pipelines (phenotypic screening, novel targets for gametocytes and liver stages) are also yielding promising leads that could become oral single-dose cures or new severe-disease treatments in the years ahead. PubMed+2scienceforafrica.foundation+2
Why this is a game-changer: new classes of medicines reduce the risk that parasites will outsmart our drugs. If a non-artemisinin combination achieves broad deployment, it would add resilience to treatment programs while stewardship and surveillance protect drug efficacy. PMC
Smarter use of existing medicines: IPTp, IPTi, and expanded preventive options
Beyond vaccines and SMC, public health programs are refining how existing antimalarials are used:
- Intermittent preventive treatment in pregnancy (IPTp) (usually sulfadoxine-pyrimethamine) continues to reduce maternal anemia, placental malaria and low birth weight. Strengthening antenatal delivery of IPTp and improving uptake in pregnancy clinics has clear benefits for newborn survival.
- Intermittent preventive treatment in infants (IPTi) and school-based preventive regimens are being studied or deployed in targeted settings to reduce child morbidity.
- Dihydroartemisinin–piperaquine (DHA-PQ) has been trialled as an alternative SMC choice and for expanded seasonal regimens in places where SP+AQ loses potency; adaptive deployment of these regimens is informing country policies. The Lancet+1
The lesson: combining smart, evidence-driven use of established drugs with new tools multiplies impact, particularly when choices are adapted to local seasonal patterns and parasite resistance profiles.
Improved diagnostics and drug delivery: getting the right medicine to the right person
Medicines save lives only when the right patients receive them quickly. Africa has seen rapid scale-up of rapid diagnostic tests (RDTs), which allow reliable malaria diagnosis outside hospitals and reduce inappropriate use of antimalarials. Coupled with strengthened supply chains, community health worker programs, and private-sector engagement, diagnostics let health systems target therapeutics—preserving drug efficacy, reducing waste, and lowering costs.
Point-of-care testing plus algorithms that triage febrile illness (i.e., testing before treating) has also improved surveillance data, giving programs better real-time signals for outbreaks and drug efficacy monitoring. These feedback loops are essential for early detection of emerging resistance and for choosing where to deploy new medicines or switch regimens. (See WHO and national programs for examples.) World Health Organization
Better bed nets and integrated vector control complement medicines
Modern medicines are most effective when combined with vector control. The rise of insecticide resistance has degraded the protection offered by older pyrethroid-only nets, but scientific innovation has yielded a new generation of nets treated with dual or multi-active insecticides (e.g., pyrethroid + chlorfenapyr or pyrethroid + pyriproxyfen). Large multicountry trials across Africa showed the new nets can reduce malaria by significantly larger margins than older nets, and programs are rolling them out in high-burden settings. That reduction in transmission lowers the overall burden and makes medicines and vaccines more impactful. The Guardian+1
Integrated vector control—targeted indoor residual spraying, larval source management where feasible, and environmental measures—keeps mosquito populations down and reduces the number of infections that medicines must treat. The synergy between modern nets and modern medicines is a central reason progress is possible. The Guardian
Local manufacturing, partnerships and access: getting modern medicines into African hands
A historic challenge has been affordability and accessibility. But recent policy shifts, partnerships and manufacturing initiatives are making modern medicines and vaccines more available in Africa:
- International donors (Global Fund, Gavi, Unitaid and others) subsidize procurement and help countries adopt new tools.
- Public–private partnerships have accelerated trials, manufacturing commitments, and access plans for new drugs and vaccines.
- Some multinational manufacturers and regional players are planning or expanding local production for antimalarials, drug formulations and vaccine components—shortening supply lines and reducing costs over time.
These financing and production strategies are crucial: new drugs that sit in labs are no use unless countries can procure and deliver them to clinics and communities. World Health Organization+1
Evidence from the field: what success looks like
Success is visible in multiple ways:
- Fewer severe cases and deaths where the vaccine and SMC are well implemented. Pilot countries that introduced RTS,S alongside strengthened treatment and prevention have reported declines in severe paediatric malaria admissions where coverage is high. The combined approach—vaccination, SMC, bed nets, testing and prompt treatment—reduces child mortality and health system strain. World Health Organization+1
- Lower seasonal surges in SMC areas. In places where SMC cycles reach high coverage annually, hospital admissions among the under-5s during peak months fall substantially compared with non-SMC areas. Operational studies and meta-analyses confirm the strategy’s effectiveness at scale. Am J Trop Med Hyg
- Clinical trial success for new treatments. The ganaplacide + lumefantrine combination—tested in children and adults—met efficacy endpoints in recent trials and is now in Phase III studies; that progress materially strengthens the pipeline against resistance. scienceforafrica.foundation+1
These field results show modern medicines, when combined and properly delivered, shift outcomes materially toward fewer child deaths and fewer severe illnesses.
Real challenges that require continued investment
The optimism must be balanced with reality. WHO’s 2024 World Malaria Report and global news coverage underline several hard truths: after dramatic gains in the 2000s and early 2010s, progress has slowed; cases rose again in recent years in part because of funding shortfalls, climate-related and humanitarian crises, and the creeping specter of drug and insecticide resistance. To sustain and accelerate the gains from modern medicines, the continent needs predictable financing, stronger supply chains, and scaled health systems that reach remote and conflict-affected populations. World Health Organization+1
Key constraints include:
- Funding gaps. WHO estimated billions more are needed annually to reach global targets; donor fatigue or diverted budgets undermine program continuity. World Health Organization
- Resistance monitoring and stewardship. Rolling out new drugs demands simultaneous surveillance to detect resistance quickly, plus policies to steward new medicines so efficacy isn’t lost. PMC
- Logistics & workforce. Vaccines and chemoprevention require reliable cold chains, community health workers, and supply management—areas that need continual investment. World Health Organization
What governments, donors and communities can do next
To consolidate and accelerate wins, coordinated action is required at multiple levels:
- Scale evidence-based tools where they work: rapidly expand vaccine programs in eligible countries, increase SMC campaigns in seasonal zones, and deploy next-generation bed nets to replacement campaigns. World Health Organization+1
- Fund the pipeline and procurement: ensure predictable financing for procurement of vaccines, new drugs and nets, and support local manufacturing where possible. World Health Organization+1
- Invest in surveillance and stewardship: maintain and expand molecular surveillance for drug resistance, commit to rotating or combining therapies thoughtfully, and monitor insecticide resistance to guide vector control choices. PMC+1
- Strengthen health systems: train and pay community health workers, improve diagnostics access, and embed malaria services into routine maternal and child health platforms. World Health Organization
- Support research translation: accelerate regulatory processes for promising new antimalarials, but pair approvals with access plans so medicines reach clinics quickly. scienceforafrica.foundation
A realistic but hopeful outlook
Is Africa “winning” the battle against malaria? The honest answer is nuanced. On one hand, modern medicines—vaccines, smarter chemoprevention, and a deep pipeline of new antimalarials—are the strongest and most durable weapons humanity has ever had against malaria. They are already saving lives where they are used effectively. On the other hand, progress is fragile: innovations must be paired with funding, robust delivery systems and vigilant resistance monitoring or gains can be lost.
The turning point is that the tools now exist to make major, durable reductions in malaria’s toll—particularly among children. The next five to ten years will be decisive: they will determine whether new medicines and vaccines become standard of care across the continent, and whether Africa can translate scientific breakthroughs into population-level declines in cases and deaths. With the right investments in finance, supply chains, and human resources, the combination of modern medicines and smarter public health can — and likely will — tilt the balance decisively in Africa’s favor. World Health Organization+2World Health Organization+2
Quick facts (snapshot)
- Estimated global malaria cases in 2023: ~263 million; malaria deaths ~597,000 (majority in Africa). Progress since 2000 has averted billions of cases and millions of deaths, but recent years saw a rebound in cases in some regions. World Health Organization
- RTS,S: first vaccine recommended by WHO for children at risk (rollouts in Ghana, Kenya, Malawi and expanding). R21: another vaccine candidate showing promising results and being introduced in additional settings. Vaccines complement, but don’t replace, nets and medicines. World Health Organization+1
- SMC: proven preventive drug cycles for young children during seasonal peaks—used widely across the Sahel with large reductions in child illness where coverage is high. Malaria Consortium+1
- New drug candidates (e.g., ganaplacide, cipargamin) offer alternative mechanisms to protect against resistance and treat severe disease; some are in Phase III or late development. scienceforafrica.foundation+1
Closing — medicine plus systems: the winning formula
The story of malaria in Africa is no longer one only of failure or inevitable tragedy. It is increasingly a story of scientific success translated—when policy, funding and delivery align—into saved lives. Modern medicines (vaccines, chemoprevention, new antimalarial classes) are turning the tide, but to claim a decisive and lasting victory requires sustained investment, adaptive policy and the political will to make these tools available to every child, pregnant woman and family at risk.
If governments, donors, researchers and communities keep the focus on integrated delivery—vaccines and SMC widely available, diagnostics and drugs in stock, resistance monitored in near real-time, and new drugs deployed intelligently—then the phrase “winning the battle” will become less an aspiration and more an accurate description of the next chapter in Africa’s public-health story.







{kind=link}